Examination protocols with MagniXene® yield images, usually in three dimension. Xemed is working with clinical researchers and image processing scientists to refine methods for using these images to quantify metrics that determine disease phenotype or severity status.
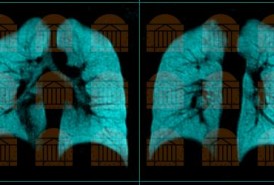
Ventilation: The most extensively studied and most broadly applicable protocols for hyperpolarized noble gas MRI exploit its use as a tracer gas for pulmonary ventilation. In addition to three-dimensional high-resolution maps of gas distribution during a single breath hold, researchers have demonstrated movies of inhalation and exhalation and multiple breath build-ups and wash-outs of gas concentrations. Ventilation maps have been applied to staging and phenotyping COPD, asthma, cystic fibrosis, bronchiolitis obliterans, radiation-induced lung injury, and other respiratory conditions.
Alveolar size: Alveolar septal walls divide the lung gas space, restricting the distance scale of gaseous diffusion. MRI protocols sensitized for diffusion are able to quantify the average distances of diffusive transport, represented as an apparent diffusion coefficient (ADC). Maps of the degeneration of septal tissues allow phenotyping of emphysema, an important subcategory of COPD. Histograms of ADC values quantify disease severity.
Emerging protocols that characterize regional disease by interrogating the gas:
Small airway dimension: Physical barriers can limit diffusion in all three dimensions, albeit at different length scales. Several approaches (kurtosis, 6b-ADC, q-space imaging) have demonstrated sensitivity to quantifying an additional spatial constraint on acinar diffusion as the diameter of the smallest associated airway.
Collateral ventilation pathways: Studies of gaseous diffusion find continuing migration even at anomalously long times. This long-range component, which is not consistent with diffusion along a branched structure, is interpreted as collateral ventilation between airway branches. Lung regions with high values of long-range diffusion appear as early pre-symptomatic changes in long-term cigarette smokers, which may lead to emphysema.
Alveolar oxygen/perfusion: Hyperpolarized gases lose their magnetic enhancement at a rate that depends on the local concentration of oxygen. This property is exploited in the lungs to determine regional rates of perfusion and oxygen uptake from the lung gases. Noninvasive regional oxygen measurements could be useful in development of drugs for conditions that obstruct blood flow (pulmonary arterial hypertension PAH) or limit gas exchange (idiopathic pulmonary fibrosis IPF).
Emerging protocols that characterize regional disease by interrogating the dissolved phase:
Alveolar S/V: The magnetic resonance frequency of xenon-129 in the dissolved phase exhibits a shift of roughly 200ppm from that of the gas phase. MRI protocols can interrogate the relative occupations of MagniXene® in these two phases to determine physiological quantities related to the surface-to-volume ratio of the acinus. This dimensional parameter could be useful for quantifying progression of emphysema.
Septal wall thickness, inflammation: MagniXene® appearing in the dissolved phase achieves an equilibrium concentration through continuous fast exchange with MagniXene® in the gas phase. If the dissolved phase magnetization is quenched, it will recover to its equilibrium partition over a period of time that depends on its composition and geometry, especially its thickness. Time-dependent measurements of MagniXene® saturation can be used for development of drugs to reduce inflammation in COPD or to halt fibrotic activity in IPF.
Exchange with red blood cells: The magnetic resonance frequency of xenon-129 in hemoglobin exhibits a signature shift of 210-215ppm from that of the gas phase. Pharmaceutical companies could utilize regional maps of the exposure of inhaled MagniXene® to red blood cells, exhibiting regional variations that are associated with hypertension or vasoconstriction.
